

The covid-driven backlog of planned surgery patients still hasn’t been cleared. Almost 4000 remain in limbo.
Less than a quarter of NSW local health districts reported zero overdue planned surgery patients in 2024-25, and the significant backlog from the covid pandemic still has not been cleared, a new report from the Audit Office of NSW says.
“NSW Health has cleared most of the backlog of patients waiting for surgery caused by pauses to planned surgery during covid,” the report said.
“However, it is not meeting the nationally agreed target of ‘zero patients waiting longer than clinically recommended for surgery’.”
Planned surgery was paused several times between March 2020 and January 2022 – the peak of the covid pandemic – with overdue patient numbers reaching a peak of almost 19,000 in April 2022.
In the pre-covid year of 2018-19 there were around 1000 overdue planned surgery patients across the state, and the Ministry of Health views that year as a benchmark against which to measure performance, the report said.
Between January 2022 and December 2025, NSW Health trialled initiatives including surgical hubs, pooled surgery waitlists and reducing unnecessary surgical interventions, but those initiatives have not been rolled out across NSW, the report said.
More than 230,000 elective surgeries were performed in NSW in 2024-25 with a total cost of $2.3 billion.
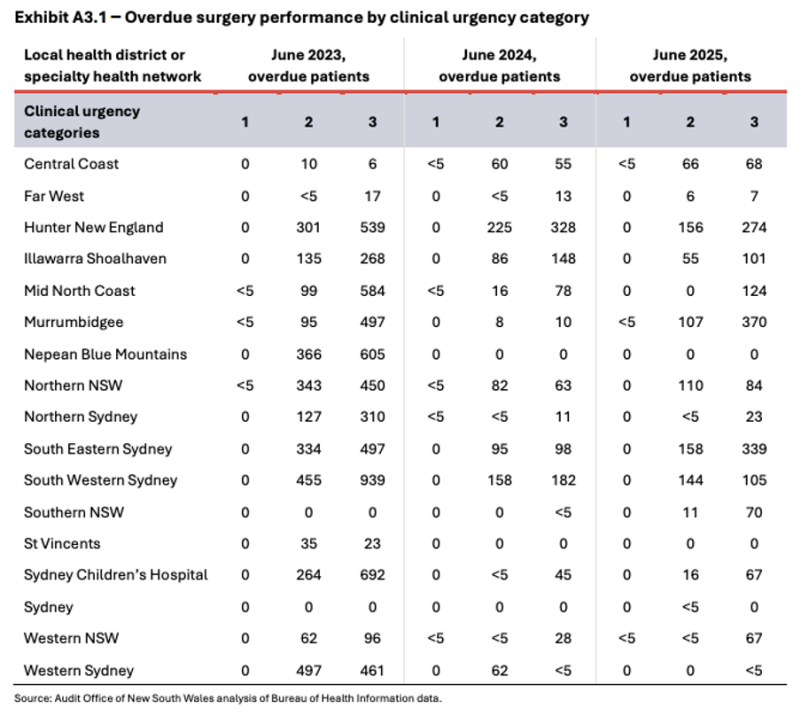
The report’s breakdown of LHD waiting lists shows that South Eastern Sydney LHD tops the bad news list with the highest number of overdue planned surgery patients.
At the end of the audit period in December 2025 there were almost 3900 overdue patients statewide, the report said.
Also in today’s edition:
“In 2024-25, only four of the 17 LHDs and specialty health networks met the goal of zero patients waiting longer than clinically recommended for surgery,” the report said.
Figures for June 2025 show that the LHDs with the highest numbers of overdue planned surgery patients – including all three urgency categories – were South Eastern Sydney (497), Murrumbidgee (477), Hunter New England (430) and South Western Sydney (249).
South Western Sydney and Hunter New England LHDs underperformed on planned surgery access KPIs, the report said, and both have had pressure on planned surgery capacity including unplanned demand, infrastructure constraints and clinical workforce shortages.
When surgery data was broken down into urgency types, the highest numbers of overdue category two patients – surgery to be performed within 90 days – were in South Eastern Sydney (158), Hunter New England (156) and South Western Sydney (144).
The audit made three recommendations to NSW Health:
- Define additional efficiency performance targets for inclusion in service agreements with local health districts.
- Identify and determine the planned surgery service delivery models that achieve greater efficiencies and surgical throughput, and target policy and investment accordingly.
- Develop additional risk-based guidance for local health districts to conduct regular reviews of waitlist management and compliance.
Related



A response from NSW Health secretary Susan Pearce, published with the report, said the reductions of planned surgery waiting times had been a significant focus for NSW Health since planned surgery was paused during covid.
“I am pleased to see the outcomes of this work reflected in this audit report and affirm that the monitoring of waiting times will remain a focus,” she said.
Ms Pearce said it was important to note that planned surgeries were prioritised according to the clinical urgency category timeframe, which is allocated by the treating doctor.
“Only the treating doctor or delegate can change this timeframe, based on objective clinical evidence.
“The scheduling of patients is undertaken in consultation with the treating surgeon, to ensure that patients with the greatest clinical need are prioritised.”
Ms Pearce said urgent surgery took precedence over other patients and may delay planned surgery.
“This may impact on the interpretation of performance data,” she said.
“A decision to postpone surgery is only made after all other options are exhausted and following consultation with the treating doctor.
“The choice of the patient is also a critical factor in this decision and where the option to postpone surgery is taken, it is rescheduled as quickly as possible.”
Ms Pearce said NSW Health, in collaboration with LHDs and specialty networks, had been developing strategies to improve access to planned surgery, including:
- LHDs and specialty networks have secured funding to reduce overdue surgery by increasing surgery throughput by purchasing new equipment or establishing a high-volume short stay surgery program and introduce programs aimed at providing high-value, non-surgical care options to ensure timely access to appropriate care for patients.
- Providing an option for patients to have surgery sooner at another public or private hospital where clinically appropriate.
- The use of pooled lists to maximise available capacity supported with extended theatre sessions where workforce and clinical appropriateness allow.
- Completion of a series of waitlist policy compliance audits.
- Empowering clinicians to make evidence-based decisions for alternative treatments for some patients where surgery may not be beneficial.