

AI scribes are taking off in Australian general practice. Different survey results suggest the market is struggling to define what ‘use’ actually means but that’s not the problem for GPs and patients.
Depending on which survey you read, AI scribes are either already mainstream in Australian general practice, or still being used by fewer than one in five GPs.
Both things may be true.
The latest Healthed/HSD survey of 1535 GPs found that just 18.7% said they personally use an AI scribe for consulting, while 81.3% said they do not. Among those not using one, about one-third said they were seriously considering doing so.
At first glance, that appears sharply at odds with the RACGP’s newsGP poll, which reported AI scribe use rising from 22% in August 2024 to 40% in November 2025. The Guardian subsequently cited that figure in March this year, reporting that “two in five Australian GPs” were using AI scribes.
But the discrepancy says more about the market’s rapid and eclectic evolution than about flaws in the surveys themselves.
The key issue is probably the question being asked.
The RACGP poll asked whether respondents were “currently using artificial intelligence scribes in your general practice” (our emphasis). That wording potentially captures practice-level use — whether AI scribes are being used somewhere in the clinic, by some doctors, during some consultations, or in trial programs.
The Healthed/HSD survey asked a narrower question: “Do you use an AI scribe for consulting?”
Personal use is the harder, but more meaningful adoption metric because it strips out:
- Trial (often free) programs;
- colleague use;
- practice availability;
- and occasional experimentation.
On that basis, the best current estimate may be that active, routine AI scribe use among Australian GPs sits closer to 20% than 40%.
But that does not mean adoption is slow.
HealthEd/HSD’s survey in October 2024 found AI scribe use at roughly 8% and the question in that survey was also broad, not specific, about personal use, so the number is very likely overestimated.
If the comparable May 2026 figure is now 18.7%, adoption has more than doubled in less than two years and probably more than tripled.
That is a very steep growth curve by healthcare technology standards.
The market is probably moving through multiple stages simultaneously:
- practice-level exposure;
- experimentation;
- partial workflow adoption;
- governance development;
- and, finally embedded daily use.
The Healthed/HSD data also suggests that once doctors adopt AI scribes, many use them heavily.
Among current users:
- 37.3% said they use AI scribes in 80%-100% of consults;
- another 18.3% use them in 60%-80% of consults.
In other words, adoption appears “sticky”. Once GPs become comfortable with the workflow, many integrate scribes deeply into daily practice.
Notably as well, patient resistance isn’t a barrier.
Among AI scribe users 70.3% said 80%-100% of patients were comfortable with AI scribes being used during consultations.
The more significant constraints may instead be governance, workflow habits and patient management system integration.
Only 25.0% of respondents said their practice had an AI governance policy, while 75.0% said they did not.
Also in today’s edition:
That is a notable gap given these tools are increasingly being inserted into live clinical workflows involving privacy, consent, data handling and medico-legal responsibility around decision support.
The most important recent governance battleground is “decision support” modules being added to AI scribes.
Heidi recently announced Heidi Evidence, which is a knowledge layer that can analyse the consult summary and make recommendations or answer questions around the summary.
Lyrebird is looking closely at its own knowledge layer in the form of MedLuma, the recently released Australian-focused evidence-based knowledge base from Medcast.
The market is moving much faster than regulatory bodies can, forcing GPs to decide on how much governance they are happy with.
The Healthed/HSD survey also suggests most AI use in general practice remains focused on documentation relief rather than broader clinical decision support.
When asked which AI-based tools they used during consults for decision support:
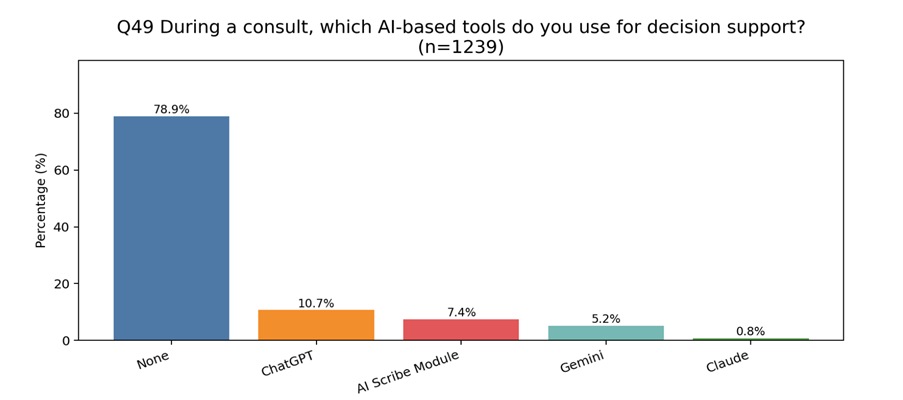
That implies most current adoption is still about reducing administrative burden rather than augmenting diagnosis or clinical reasoning.
International comparisons suggest Australia is not unusual.
In the UK, AI uptake among GPs appears to sit in a broadly similar range, although survey definitions vary there as well.
NHS England is now actively developing national frameworks for “ambient scribing” technology across the health system, while multiple UK studies suggest between 20%-30% of GPs are now using some form of AI assistance in workflow.
In the US adoption appears to be accelerating faster, particularly inside large health systems. But the numbers there can blur together as well between healthcare AI use, consumer AI use for healthcare, and AI scribe use.
What seems clear, however, is that AI scribes are moving out of the experimental phase.
The latest Heidi Health impact report for the UK claims the company now supports:
- 1.8 million appointments per month in the NHS;
- has processed 15.2 million sessions; and
- is used by “one in two UK GPs”.
Even allowing for vendor enthusiasm and varying definitions of “use”, these aren’t fringe numbers.
But the Heidi report also quietly highlights the same issue now emerging in Australian survey data: defining adoption is becoming complicated.
The report uses all these terms around adoption:
- adoption;
- activation;
- engagement;
- utilisation; and
- active use.
The report itself notes that the biggest challenge is no longer proving the technology works, but achieving “consistent, repeatable implementation”.
That may ultimately be the simplest explanation for the conflicting Australian numbers.
Related


AI scribes are no longer niche, but they are not yet fully normalised either.
A realistic interpretation of the current data could be:
- roughly one in five GPs are now active personal users;
- many of those users rely on the tools heavily;
- a much larger proportion of practices are now experimenting with, trialling or partially deploying AI scribes somewhere in workflow;
- governance issues aren’t holding anything back so far.
If this is all happening a very important question everyone should now start asking themselves is, what does this now rapidly unfolding pattern mean for non-AI using Australian GPs?
If AI scribe users are saving time, reducing after-hours documentation, improving eye contact, producing more complete notes and embedding the technology into most of their consults, then the gap between users and non-users may start to become overt before too long.
Are AI-scribe GPs becoming more efficient? Almost certainly.
Will they make more money? Possibly. If saved time translates into better throughput, less administration drag, more complete billing capture and efficiency in payments.
Will they become better doctors, qualitatively, quantitatively or both?
Better notes, better recall, more attention during the consult and less cognitive load all suggest potential upside for care quality.
But all this would need proper measurement and that’s not going to be easy.
For patients, the upside seems obvious (potentially anyway): more present doctors, better documentation, faster letters, cleaner follow-up and fewer dropped details.
But there is a distinct possibility that some demographics of GPs may simply never adopt these tools because of age, trust, cost, workflow discomfort, medico-legal anxiety, privacy concerns or philosophical opposition.
If that happens, AI scribing may not just create a productivity gap between practices. It may create a new kind of clinical and operational divide.
That is something the profession’s peak bodies need to start thinking about now, on behalf of both their doctors and their doctor’s patients.