
In healthcare we seem to have a collective delusion that prevention is a wicked, maybe even whimsical, problem, so while we pay much homage to the idea we never get too serious about trying to actually crack it. But, maybe we’re collectively deluding ourselves about how wicked it actually is
I went to the Public Health Association of Australia’s national conference this week, on a last-minute whim, hoping to gain more insight into why prevention is the word on everyone’s lips, and has been for decades, but we can’t seem to get any traction on embedding it as a key structural and well-functioning element of our system.
Very soon after arriving it became clear to me that I should have been talking to this group a long time ago for ideas.
Collectively it’s a great group of stakeholders from all walks of healthcare, with a very deep commitment to the idea of prevention, and working hard at it for a long time.
This realisation still didn’t help me a lot, though. The PHAA, in its’ current form, is 40 years old – its predecessors go back to 1936, however – but it feels like a lot of the problems it would have identified when it started are still around.
The surreal thing for me is that no one, either within this group or without, is arguing whether prevention works (although we do argue a lot over what it actually is), whether it would deliver long-term value or not, and whether we need to shift the system somehow to accommodate it better.
But after this our sector-wide delusion seems to kick in:
“Yeah, whatdya do? We’re federated, the ROI is hard to calculate, in large part because we don’t have a collective definition for it across the system, and of course, there’s the politics, which is in a three-to-four-year cycle, while prevention and its obvious ROI clearly isn’t .”
Our secretary of health, Blair Comley put it succinctly to us all in his appearance at the event when he explained that he doesn’t “have much work to do convincing the centre of government that early intervention works”.
The problem is what comes next. Inside government, every proposal runs into the same constraint:
“I believe your argument … I don’t dispute that this has got a high benefit-cost ratio. So I’d just like you to do that – and offset within your portfolio something else that’s clearly got a lower benefit-cost ratio.”
Ultimately, he says the sticking point is this:
“What I have trouble convincing them of is, why I’m not doing the prioritisation myself.”
He’s challenging stakeholders to do better in making his arguments.
Mr Comley is articulate and trying to help. He went on to outline exactly how we need to pitch to him and his colleagues.
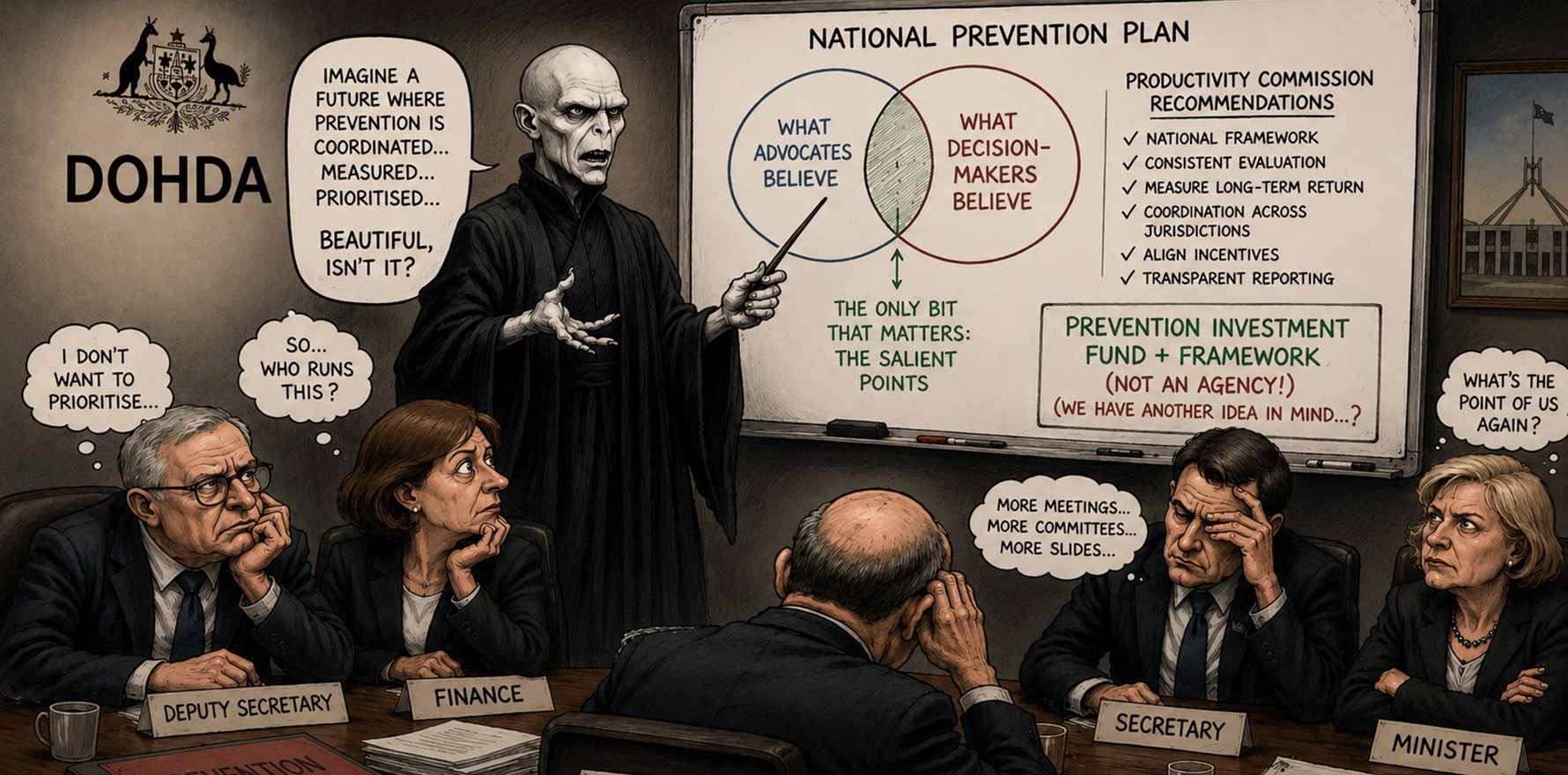
The Venn diagram problem
Comley wants us to approach him with his Venn diagram paradigm in mind. This is what he thinks:
“If you’re arguing things that you believe, but your audience doesn’t, that’s just self-indulgent.
“If you’re arguing things your audience believes but you don’t, that’s pandering.
“The only bit that matters is the overlap – the salient points.”
Blunt, but useful.
In one circle we should put what advocates believe, in the other, what decision-makers believe.
The intersection – the “salient points” – is where things get funded, he suggests.
Mr Comley’s Venn diagram paradigm, applied to prevention, exposes something fundamentally wrong with what we’ve all been doing.
At the moment advocates are arguing for better programs but government is asking for better prioritisation.
Neither addresses the structural gap between them – it’s not about ideas. It is about coordination.
Wow, nice timing everyone. Someone has just recently addressed this problem eloquently for us all.
It’s in the Productivity Commission’ss recent review Delivering quality care more efficiently.
Is the Productivity Commission being coy?
This review is recommending:
- a national framework for prevention investment;
- consistent evaluation of programs;
- measurement of long-term return;
- coordination across jurisdictions;
- alignment of incentives; and
- transparent centralised reporting.
Taken individually, these are sensible reforms. But you would not want to try to achieve any of them without a central co-ordinating body to create the obvious synergies and system workflows.
None of these functions can be delivered consistently by a collection of stakeholders operating independently, or by happy-clappy collaboration and goodwill between the jurisdictions that are in charge of delivery – the states.
No, this requires a joint jurisdictional ownership framework, authority, as much independence from politics as you can manage, and long-term continuity.
In other words, it requires a centre of gravity in some form of body.
Now we enter some very weird, I’m guessing political, territory, where I’m going to admit I have no idea what is going on.
Before I get to a very obvious point, I wonder if you as the reader disagree yet with any of the logic presented.
If you largely don’t then you, like myself, think that a key recommendation of the Productivity Commission, which it didn’t really make (it does, but vaguely) is that we need a central co-ordinating agency, funded and reporting to all the good work already being done via the various independent state agencies, and the Commonwealth, with the ability to co-ordinate investment from all points of the compass according to a nationally agreed upon plan.
The elephant in the room
Why are we not okay to say this out loud?
You cannot coordinate national prevention, measure system-wide return, align Commonwealth and state incentives and create (for Mr Comley in particular) or enforce prioritisation … without creating a body responsible for doing exactly that.
Right?
Call it what you like, but functionally, it is a national preventative health agency, not entirely like, but with very similar characteristics to the Australian Digital Health Agency, and Healthdirect.
Oh, you read this last week, right? Don’t stop reading, last week we did Treasury, this week we are doing Health. They are equally important to this idea.
Shaking our collective delusional selves out of our stupor
A couple of fun and telltale dynamics from the PHAA conference floor this week.
The first was – something I already knew because I’d asked and been told – the Productivity Commission was fairly strident in denying that it was not recommending an “agency” to do what its report had so cleverly outlined.
An observation I swear is real is that it was the word “agency” that the Productivity Commissioner Dr Alison Roberts was running a mile from, almost like she was avoiding saying “Voldemort” in a Harry Potter film.
The Structural Solution that Must Not Be Named.
So being my pesky self I got up during a really good session with the four very sharp women who are running the most important independent, but state-funded, prevention agencies in the land in Queensland, Victoria, WA and SA.
(NSW has a version of it, but it sits within the NSW Health department so it’s not what you’d call apolitical.)
I asked that given the major recommendation of the Productivity Commission report, the obvious problems with co-ordination, and how the ADHA and Healthdirect are succeeding with a cross-jurisdictional funding and reporting model, why not a federal agency of some sort for prevention?
Related



Now this was a very impressive set of healthcare executives who had just been through a very enlightening, and encouraging panel on the future of prevention – but state by state.
But it was apparent I’d asked the “Voldemort” question.
They looked at each other awkwardly, and I think knowingly (I’m just guessing of course but it felt a lot like they knew something I clearly didn’t), hoping the panellist next to them would take the question.
One of them plucked up her courage and suggested I may have been misinterpreting the review because the review didn’t recommend anything like an agency.
“I think what Alison [Roberts] was talking about is a prevention investment fund and framework … what can you nationally invest in, and how do you do that in a way that’s collaborative with the states.”
This panellist was right. The Productivity Commission didn’t recommend an “agency” model as such.
I had imputed that it had from what it recommended. How else could you do what they were recommending?
The Commission, by the way, recommended something strangely vague that sounded very apolitical … I think the PBS was mentioned as a model.
The PBS, I thought? That isn’t a particularly relevant structure to reference in this situation. That it was referenced, I felt, was clasping at straws.
I mean, if someone were to recommend the creation of the PBS today (it’s been a centrepiece of our healthcare system – next to Medicare later – for nearly 80 years thankfully, set in motion by a visionary Labor government under Chifley) you’d be laughed out of Canberra.
It certainly wouldn’t make it through Mr Comley’s Venn diagram test in today’s stressed set up.
What was going on here?
One of the panel piped up with “we’ve also got the CDC now, and its long-term remit is chronic disease prevention”.
Long term? It’s doubtful it will get ever get on top of its short-term remit.
Why was everyone stalling here?
All four highly competent state-based prevention leaders immediate reaction was to deflect the question in some way.
The question had clearly made not just them uncomfortable, but a few people in the room, I think.
As stubborn as ever, I shirtfronted two of the panelists after the session and explained in a bit more detail what I meant.
As a part of my pitch to them – a point which surely would hit that green overlap in Mr Comley’s Venn diagram – was that if you step back and analyse the upside of the ADHA and Healthdirect for the states, while the journey has been rough at times for both, the benefits for the states are starting to accrue quite significantly now.
I also said that such an institution would in effect have to be connected at the hip with them because they were at the coalface of delivery, and were a vital part of the IP of a successful national venture.
Both panelists agreed up front with me that explained this way they liked the idea.
They also said that as a group they were very tight, met regularly and tried to work collaboratively between jurisdictions.
I didn’t doubt it. They’re all women after all, and that’s what they do really well – get on with the meaningful stuff and leave the petty power stuff alone. They’re working together.
That I see as another bullseye on the green zone of Mr Comley’s Venn diagram … the state health prevention agencies are pretty much on board if you frame the solution accurately.
Why no one is objecting
What’s interesting is not that this idea exists. It’s that almost no one is actively arguing against it – especially when you provide the framework for how it operates and point to the upsides, including the pluses that have come out of the ADHA and Healthdirect for the whole system.
That’s unusual in health policy.
Normally, such significant proposed structural reform triggers immediate resistance:
- jurisdictional tension;
- funding disputes;
- bureaucratic defensiveness.
Here, that resistance is muted. Why? Because the current system is visibly broken and every stakeholder knows it.
Prevention is fragmented, investment is inconsistent, outcomes aren’t measured or are poorly measured, accountability is so diffuse it doesn’t exist, and nobody is responsible for delivery overall.
So, when the idea of coordination emerges with the right framing, it doesn’t tend to trigger opposition. It tends to trigger recognition.
The barrier isn’t politics this time either
I’m going to suggest that the idea that this is politically difficult is a part of the delusion and stupor I’ve referred to earlier in this article.
The ADHA and Healthdirect are both jointly funded and governed and designed specifically for cross-jurisdiction management
The model exists, albeit it’s not perfect in any way.
The barrier is not “can we do this?” It’s more subtle.
Like, no one has quite forced the system to acknowledge that we are all describing and seeking the same thing. We’ve run on the field and we’ve all got the same uniform on.
The difference between Treasury and Health
Anyone wondering if I just took my op-ed from last week and asked my AI to do the same story this week, but this time try to convince Blair Comley to play ball, well, I sort of did.
But with good reason.
From Treasury’s perspective – the Jim Chalmers frame – prevention is an investment question: what’s the return, what are the trade-offs, measure it, so we can firmly identify the savings and define the productivity questions.
From Health’s perspective – the Comley Venn diagram frame – it’s a system question: who delivers this, how is it co-ordinated, how do we prioritise with system complexity, and, an overlapping Treasury question, who pays for it?
As I said last week, this problem belongs as much in Treasury as it does Health. Unfortunately, they don’t talk enough.
I wonder if they can join forces on this one given the clear upside and the low degree of difficulty of getting the idea up.
Because prevention sits in the overlap and in that overlap the absence of structure is our problem.
Why better pitching won’t solve this
Mr Comley is right to challenge stakeholders. Most prevention pitches don’t identify trade-offs, don’t align to system priorities and so don’t land with decision-makers.
But even if every pitch improved overnight, the system would still struggle, you suspect.
The core issue isn’t just the quality of ideas, it’s the lack of a mechanism to receive them, evaluate them, co-ordinate them and scale them.
This isn’t a just a communications issue, it’s an institutional issue.
Mr Comley runs an internal shark tank at the DoHDA where his managers pitch their ideas to him and a few others at regular intervals.
Maybe he needs an outward facing version of the same pitch event from time to time?
What an agency would actually do
I did this last week but it’s worth repeating. Repetition (frequency) is how advertising works after all.
Strip away the politics, and the role is straightforward. A national preventative health agency would:
- review the national landscape and map initiatives;
- create a 10 year plan, agreed upon by all the states;
- in that plan the good would rise to the top and the bad would be shelved (creating the agencies own investment fund);
- set investment priorities, co-ordinating and optimising both existing Commonwealth and state funding;
- evaluate programs going forward using consistent published frameworks;
- measure return at a system level in the short, medium and long term;
- and report transparently on outcomes.
Why this is a “no-brainer” – even one Mr Comley might go for
There’s a line way overused in prevention debates: “it’s a no-brainer”.
It’s one that Mr Comly uses to illustrate why so many pitches for funding fail … so it’s a bit of marked term.
But here goes anyway.
The reality is that if this idea – own up, Productivity Commission it is your idea – were as simple as this article, it would have happened.
So what has changed that might make the idea one whose time is nigh?
It might not be easy but every serious analysis of this problem is pointing to it.
The most cogent recent analysis is the Productivity Commission review, but everyone under the waterline that doesn’t want to politic too much on it, sees it and wants it.
We’re just not naming it. Again … weird.
The Very Obvious Policy Idea That Shall Not Be Named.
One quick last no-brainer thing. It’s all self-funding, if you think it through. See last week’s suggestion of tightening up both the ADHA and Healthdirect as a result of AI to find the starting money. In the age of AI there’s easy money in both to spare going forward.
Also, can someone pull back the random tender DoHDA just put out asking for random stakeholders to come up with random projects to manage chronic care better (no, randomly) in Australia. That’s throwing money into the wind.
After the agency works out what existing spend is good, what is bad, and what is overlap most of your ongoing funding is there in front of us all. No more likely required, at least to prove out this new initiative.
There’s a big risk in not saying this out loud now
The longer this problem remains implicit, the longer the system will obfuscate and go on funding disconnected initiatives, and have us all literally running around like proverbial headless chickens squawking about how terrible the funding set-up for prevention is.
Blair Comley is right in a few respects.
Prevention doesn’t fail because government doesn’t believe in it. It fails because of prioritisation, trade-offs and execution.
But step back a sec, look at the whiteboard and the Venn diagram you’ve just filled in for Mr Comley, and a clearer conclusion emerges.
The system is being asked to do something it was never designed to do, over and over again.
No one is loving Prevention Groundhog Day.
If as a system stakeholder you are interested in contributing ideas to this topic and getting an Australian Preventative Health Agency up and running, please come to Health Services Daily’s Canberra Health Leadership Workshop and Summit on Prevention on 16 and 17 June at the Hyatt in Canberra. The first five delegates to use this discount code will get a 50% discount on any ticket type: Extra50. If you’re reading this Jim, your ticket is on us.Program and tickets HERE.