

Private sector heavyweights unite to condemn state ‘addiction’ to revenue from privately insured patients. The feds must fend them off, they say.
Public hospitals and state governments should no longer receive federal funding for private-in-public activity, say two of the biggest names in the private health sector.
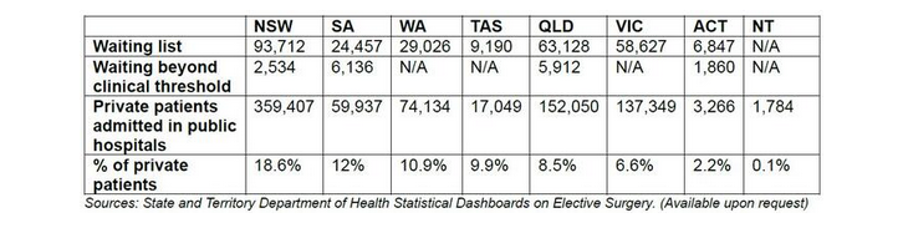
Catholic Health Australia and the Australian Private Hospitals Association have used state government data to highlight just how many privately insured patients are being treated in public hospitals.
“There are 284,987 public patients languishing on public hospital waiting lists across the country,” said a joint statement from the two organisations.
“More than 16,000 patients, that we know of, are waiting beyond the clinical threshold for the treatments they need.
“But over the last year public hospitals admitted 804,976 private patients.
“A decade ago, only 7% of patients treated in public hospitals were classified as private. Today, that figure has climbed to 11% nationally. The latest state-by-state numbers paint a stark reality.”
Last week, writing for HSD, Dr Katharine Bassett, CHA’s director of health policy, wrote:
“Under the National Health Reform Agreement, when a privately insured patient is treated in a public hospital, the Commonwealth’s activity-based funding is discounted to reflect the money expected from Medicare and the private insurer.
“On paper, this ensures financial neutrality, as the hospital should receive roughly the same total revenue whether the patient is public or private.
“In practice, the neutrality is an illusion.
“Because the Commonwealth offsets its funding through Medicare while the state’s share simply shrinks with the discount, the states save real money – collectively, around a billion dollars a year – every time an insured patient opts for public care.
“The result is a system that quietly rewards states for drawing private patients into public hospitals, not for serving those most in need of care.”
Yesterday the CHA and the APHA called on the federal government to “strengthen its hand” in the current National Health Reform Agreement negotiations.
“Public hospitals and state governments should no longer receive federal funding for private-in-public activity,” said the joint statement.
“If state-run public hospitals admit private patients, they should shoulder the gap between what Medicare and insurers pay, instead of passing it onto the taxpayer.
“The last five-year agreement saw taxpayers pay some $400 billion for public hospitals and their patient loads.
“The next agreement should come with the caveat that public patients, especially those that cross the line for their clinical wellbeing, should immediately be transferred and treated in a private hospital at the state’s expense.”
Brett Heffernan, CEO of the APHA, said it was “no secret that state governments are addicted to the revenue they receive from privately insured patients”.
Related



“If state governments prioritised public patients, waiting lists might soon not exist and ramping could be a thing of the past as more beds are freed up from those jumping the queue,” he said.
“When so many public patients are pushed to the back of the queue and are waiting longer than necessary for their surgery, it becomes very hard to justify.
“It’s not unreasonable for the Federal government to insist that public patients no longer be second-class citizens and hold states who continue to rack up disproportionate private patient caseloads to account.
“These measures may motivate state governments to pay more than lip-service to public hospital waiting lists.”
Dr Bassett doubled down on her written article for HSD:
“Public hospitals were founded on the principle of need, not entitlement. They are meant to help people who need them most – not those who have the money and status to jump the queue,” she said.
“The more this happens, the more the balance of our health system breaks down. Public patients wait longer while private hospitals struggle to remain viable.
“The incentives drawing private patients into public wards must be wound back. Public hospitals and state governments should no longer receive Commonwealth funding under the National Health Reform Agreement for private-in-public activity.
“That way, if public hospitals and states decide to admit private patients, they could no longer claim and pocket extra funding on top of what Medicare and insurers pay.”