

Australia’s healthcare system is being quietly rewired — not by a single national platform, but by the convergence of newly forming AI front doors, web based workflow networks and AI orchestration layers. The national HIE might be redundant before it even gets to tender.
Earlier this year Amazon Connect Health completed a pilot with UC San Diego Health, which, while on a distant shore, in a health system which planners in Australia love to denigrate because of its wicked payments regime, might represent the future of health institution patient engagement at scale in Australia.
It might not be that local hospital groups, or organisations like HealthDirect, use the Amazon product themselves – Amazon Connect Health.
But no Australian health institution dealing at scale with patients will be able to ignore what Amazon has now shown the new AI agents can do at scale in the UC San Diego Health experiment: EMR linked agentic patient verification, appointment management, patient insights, ambient documentation, and medical coding, all in real time.
The UC San Diego Health project, if nothing else, has proven that in days, not months of integration work at a big provider, an AI engagement agent can give patients faster access to care, clinicians more time for care, and release a conga line of related patient facing staff to do other important work.
Amazon Connect Health– yet to be formally launched in Australia but it’s coming soon – is a digital patient engagement engine that sits at the front of a health system, talks directly to a core EMR if there is one, and works intelligently in real time for a patient.
The UC San Diego Health instance is deeply integrated into Epic and “combines conversational AI with orchestration logic”.
Like me, you might ask here “que…orchestration logic, what does that mean?” – I did after all type the orchestration bit straight off an Amazon press release (better than AI making it up I guess). Read on, I think I’ve worked it out.
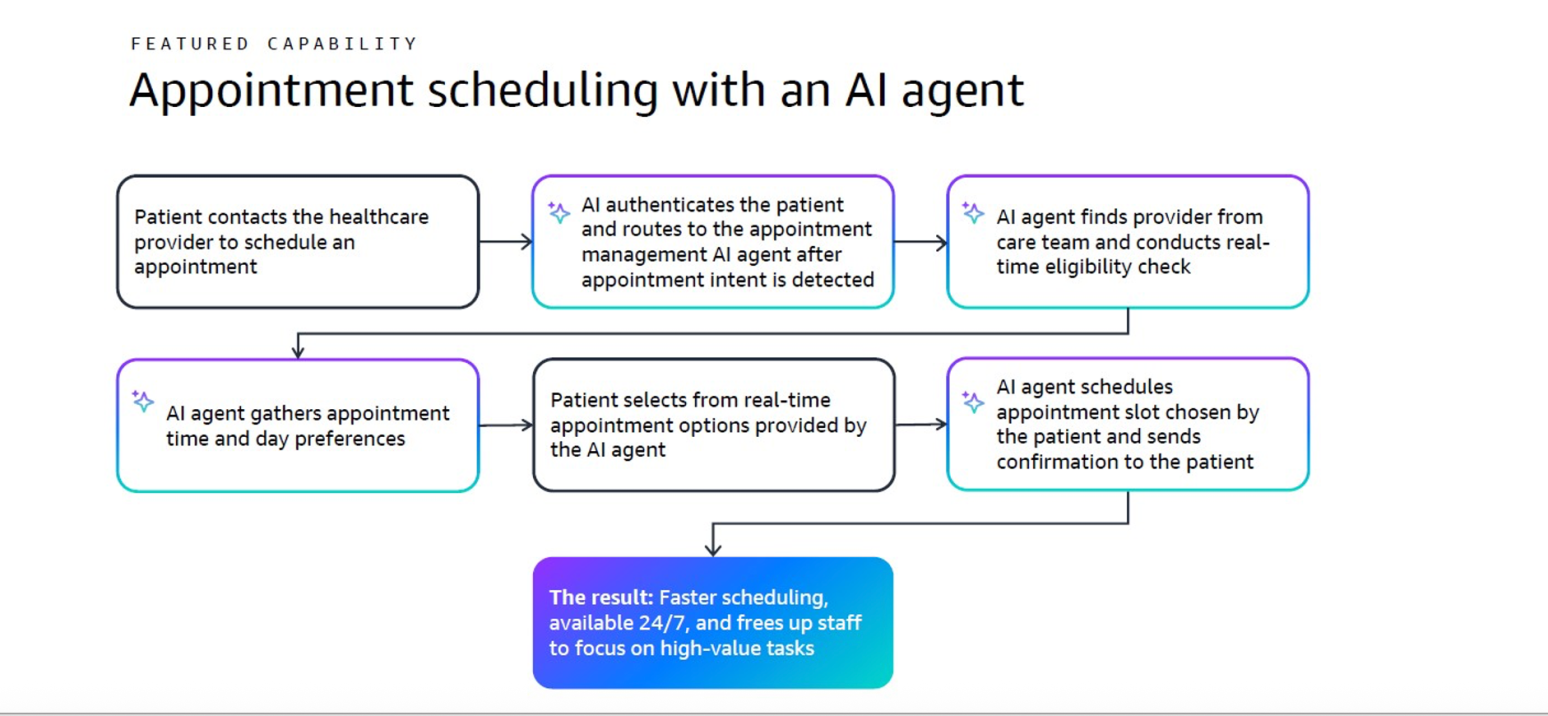
When a patient makes contact to a large provider organisation — by phone, message or web — the system verifies their identity, can understand their intent, and then can act across clinical and administrative workflows of the institution in real time. Stuff like, checking an existing appointment, booking a new one, routing the patient to the right hospital or external specialist or service, or even, resolving a low acuity query without human intervention.

By pre-verifying patients and automating common tasks Amazon Connect Health has reduced handling times, lowered call abandonment rates, and enabled 24/7 access to scheduling at UC San Diego.
According to AWS Healthcare Industry Lead, Dr Jill Freyne, it is saving around a minute per interaction.
What’s the significance of that?
UC San Diego Health is pretty big and complex. It has 13,493 staff, 1,101 beds, 36,130 annual admissions, 1.29 million annual outpatient visits and surgeries and 45 patient contact centres manned by 750 contact centre agents taking 3.2 million calls per year.
That seemingly innocuous one minute over one year translates to about:
- 300,000 staff hours saved
- 82% of patients and caregivers being self verified before reaching staff
- An 81% improvement in agent connection time, and
- A 29% reduction (on average) reduction in abandonment rate, a rate which was as high as 59% in some departments.
Imagine this sort of efficiency improvement in some of our larger hospitals in Australia.
Dr Freyne is excited about the opportunity for Australia but she is quick to say that the real shift is here is structural, not operational. That is, this AI agent dynamic is probably a lot bigger than it first looks in simple operational terms.
Traditionally, digital health tools have focused on answering questions — symptom checkers, portals, chatbots.
The San Diego Health model takes the next step says Dr Freyne “from understanding intent to executing outcomes. “
“The AI is not just advising patients where to go. It is helping them get there”.
A key to this functionality is the EMR integration.
This allows the AI to read and write data within pre-determined governed clinical workflows and frameworks.
“It is not a standalone AI layer,” says Dr Freyne
“It’s not answering questions. It’s taking action.
“It is embedded into the fabric of the health system itself”.”
It’s a digital engagement engine that can understand why a patient is contacting the system, verify who they are, and then act inside a predetermined clinical and governance framework to take that patient on a journey into and out of the system.
Where this model fits into Australia
Outside of payments, Australia has most of the ingredients of the UC San Diego Health set up in various parts of our highly fragmented provider delivery system.
Big hospitals are a clear use case. Especially to start with, ones using Epic and Cerner, of which we have quite a few in play now.
In the case of some organisations, HealthDirect as an interesting example, albeit it doesn’t operate with a patients EHR (yet…maybe the The My Health Record will be in there soon?), the fit seems particularly neat.
From a state hospital perspective, in NSW, parts of Victoria and maybe soon Tasmania, Epic is scaling across public hospitals. In Queensland, Cerner (Oracle Health) plays a similar role.
That would make the San Diego Health model – AI sitting on top of an EMR verifying patients, checking appointments, managing referrals and routing workflows — transferable for use cases such as outpatient booking and rescheduling, referral tracking, pre-admission and discharge co-ordination and specialist clinic triage.
Of course, if you’re installing Epic, or trying to tame it, who has the money to put a smart front end on your hospital?
If you talk to anyone in NSW Health there’s apparently no money for anything other than the implementation of the SDPR (which is code for the new Epic instance).
The question for state governments should then be, given the potential ROI here, and patient experience transformation, can the states afford not to engage with these new front end AI agents?
In the case of NSW, which seems to be bogged down in its Epic journey before it has even really started, maybe the leadership should stop and think for a minute whether it’s a new EMR they need across the state, or a product like the one AWS has just proven out in the UC San Diego health system.
But hospitals and our patient front doors as they exist today are only part of complex story in Australia.
Here, the real fragmentation is not inside hospitals — it’s between them and between them and primary, specialist care and other community health organisations.
Interoperability by stealth
Starting oh, so slowly – because if it’s made in Australia, hospitals have traditionally felt the technology can’t be smart enough, scalable enough or have sufficient capital backing to insure against risk ( a classic management “only buy IBM” issue) — Consultmed has slowly but surely built somewhat of a cult following among some increasingly large and important reference hospitals and hospital networks for its cloud-based advice and guidance and referral platform.
Last week the group announced its biggest deal to date, a contract to deliver e-referral and advice and guidance services to the Gippsland Health Alliance in Victoria, covering nine hospitals across the region.
The group is also in the running for Monash Health’s eReferral tender, against the traditional secure messaging providers. Consultmed connects local GPs, specialists and hospitals into a web-based shared referral and advice network. It is integrated into GP PMSs Best Practice and MedicalDirector, so in a sense, it is, by stealth, connecting hospitals to GPs. It’s also integrated to Gentu – the cloud version of market-leading specialist PMS Genie Solutions – so it’s connecting GPs to specialists to hospitals.
Prior to Consultmed these connections were made mainly, either by fax, or by point-to-point secure messaging systems. Both don’t allow networked notification to all stakeholders or asynchronous communication.
By connecting GPs, specialists and hospitals into a shared referral and advice network, it is quietly stitching together the patient journey across regions and across health networks.
And it is starting to do it at scale.
Consultmed is now:
- deployed or being deployed in around a third of Victoria’s major hospitals;
- deployed statewide in Queensland for advice and guidance;
- active in four NSW LHDs despite NSW spending about $20m five years ago on its own bespoke secure messaging solution Engage.
As Consultmed founder Dr Vikram Palit puts it:
“You can’t build interoperability with one-to-one messaging. Each message is isolated. You never actually connect the system.”
Consultmed is building something closer to a connected network.
A GP refers, or seeks advice and guidance from a specialist or hospital, a hospital receives, a specialist reviews, advice or referrals flow back, and care can be adjusted in close to real time locally.
No fax. No retyping. No restarting the process. No lost or misplaced messaging.
Possibly most importantly Consultmed, which was originally modelled on advice and guidance systems in the NHS, is providingGPs and specialists with the utility of advice and guidance.
“Advice and guidance” is when a GP or a specialist in a hospital is thinking of a referral but first does a quick digitally enabled check with a specialist – literally for advice and guidance, prior to defaulting to a referral.
In the UK, advice and guidance has been proven to stop unnecessary referrals at the rate of two out of three. In the past couple of weeks the NHS has controversially decided to enforce advice and guidance in 10 specialities.
If Australia achieved a ratio of avoiding two in three referrals, savings to doctors in time and frustration would be eye-wateringly high.
Patients would be far better off as well.
But as things go, the Australian system provides no incentive for any doctor to seek advice and guidance to make their patients journey easier, other than them wanting to save themselves time and frustration and do a better job for the patient.
In this respect the system is starting to get quite a bit of traction regardless of funding incentives.
But imagine if the government worked out a way to reward a GP or specialist to avoid two in three referrals via the “advice and guidance” network that Consultmed is starting to build?
This is technology the government should be taking quite a bit more seriously now.
As the Consultmed network of hospitals grows, and GPs and specialists become familiar with it – it also does referrals for mental and community health groups through PHNs – it looks like regions are starting to see a network effect in the deployments. The more connection, the doctors in a region realise the utility and start using it, the more powerful the network becomes. The bigger it gets the better it gets.
In Australia, acting across the system requires referral acceptance, triage between services and clinical advice before escalation
Which means the real question is not: “Can we book this patient?” It’s: “Should this patient even be referred?”
As Dr Palit puts it:
“The inefficiency isn’t booking — it’s everything that happens before a patient is accepted into care.”
This is where advice and guidance becomes critical.
In Queensland, a statewide model already allows GPs to request specialist advice — often avoiding referral entirely. Two-thirds of cases can be managed without the patient ever entering a hospital waitlist.
That is not marginal efficiency. That is system-level demand reduction and efficiency.
A rapidly changing patient journey
Put the pieces together – Consultmed’s de novo nouvo network, AWS’ new institution patient navigator, and the probability that ChatGPT and Claude will emerge as the new patient front door nationally – and something new is rapidly emerging in Australia which appears to be outpacing some very good plans laid down by our Australian Digital Health Agency.
New patient-side AI agents ChatGPT and Claude Health are rapidly starting to capture patient intent.
If Healthdirect successfully manages to partner with these patient-side AI agents, which it is now putting serious time into, it can apply a relevant local framework for triage and governance.
If a GP or Healthdirect wants to push a patient to a larger hospital network then the patient might then enter the realm of an AWS-style patient orchestration engine which takes over all the institutional workflows for a patient.
Related


Or Healthdirect might push that patient first to the GP network via one of the major booking engines, HotDoc or Healthengine.
Greasing the wheels of all of this Consultmed can connect GPs and specialists to hospitals and back for either referrals, or, simple advice and guidance for system efficiency.
The patient journey becomes:
Ask ChatGPT or Claude, understand, get passed to Healthdirect for system provider guidance and governance, maybe then a booking engine for GPs, then potentially advice and guidance, or a referral network for the journey to a hospital and back, via an AWS Health Connect-type AI orchestration product for the hospital, and then all the way back again.
That would be some transformation.
Currently what we have is: search, stop, call, wait, try to book, repeat, repeat, repeat.
Critically, the system can intervene earlier.
Instead of: “You need a specialist — wait three months”, you might get: “A specialist has reviewed this — here’s how to manage it now”.
Do we still need a national HIE?
This is where Dr Palit’s expanding network and other parallel AI developments may end up creating a need for a review of our current policy thinking on major digital infrastructure.
Australia continues to circle the idea of a national health information exchange — a large, centralised infrastructure designed to connect everything, including hopefully, a modernised and accessible My Health Record.
From a project perspective the national HIE makes the My Health Record, which we didn’t exactly cover ourselves with glory building, look easy.
Asked whether if we are ready for a national HIE Dr Palit is blunt:
“If people are still referring by fax, we’re not ready for a national HIE.
“There are simpler things we can do now — referral and advice networks — that actually connect care and reduce cost.”
A horrifying amount of GP surgeries and hospitals still use a fax machine. Dr Palit might be making an important point.
It’s an uncomfortable implication for government, not withstanding, especially because the Consultmed phenomenon is already delivering for a lot of hospitals, specialists and GPs now.
And it’s growing.
Yet the national HIE isn’t really even on the drawing board.
Interoperability may not arrive through billion-dollar infrastructure.
It may arrive through referral networks like Consultmed, workflow integration like AWS Health Connect, and a much more effective consumer front door which combines the new patient-side AI agents with Healthdirect and the booking engines.
And, incremental adoption, not a giant infrastructure project – in other words, interoperability by stealth.
And feasibly with quite a bit less risk.
Healthdirect and booking engines move down the stack
In this model, Healthdirect and the booking engines don’t actually disappear. Not to start with at least.
If patient-side AI becomes the entry point — and that seems increasingly likely — then Healthdirect becomes the clinical safety layer as the policy and governance engine of government, inserted into the process.
Looking at it another way it will be a safety framework that provides national context and protects the patients on behalf of government.
HealthDirect’s IP and data will sit inside or behind a ChatGPT ensuring that after the patient gets their health advice what happens next is safe, appropriate and compliant.
In this way HealthDirect won’t be going away.
But … it won’t be the front door anymore.
It will, not withstanding, be the component that makes walking through the front door safe for Australians.
If ChatGPT or Claude Health don’t buy that pitch, then you’d have to think they are up to something so bad the government might need to go feral regulatory on them.
They won’t want that surely.
ChatGPT got a look at this article. I wonder if it is passing it on to its boss?
And what about those $250m booking engines?
Today, platforms like HotDoc and Healthengine are essentially front doors like Healthdirect, but with a unique differentiating direct booking and branding relationship with most of our GP and allied health practices.
Potentia – the PE firm that acquired HotDoc – didn’t pay $250 million earlier this year for HotDoc to be disintermediated by AI, Google or any other emerging major global online consumer platform in the near term, surely.
The owners of these platforms feel they have some protection in that a significant proportion of their users access them through their app, not the web, and the data they hold on patients over the last 10 years is so significant it would be very hard for a new front door owner to replicate.
As well as this the booking engines will try madly to push new AI engagement tools through their distribution and branding lock, while they have it to keep secure moving forward.
The problem they are going to have of course is the problem that Healthdirect has already decided it can’t fight.
If there is enough utility in the new AI patient engines, they will slowly (maybe not so slowly) but surely, become the default digital front door, not the booking engines.
When they are no longer the starting point the dynamics for the booking engines start to warp in ways that may not be so good in the longer term because they naturally lose control, branding and pricing power.
If the system already knows what the patient needs, where the patient should go and whether a referral is even required then the booking becomes execution, not discovery.
The booking engines aren’t going to disappear even if this occurs. Their data and IP should make them a component in the patient journey for a long time still, but one that is some sort of integration to either Healthdirect or the patient-side AI engines.
But like HealthDirect, not one that is the front door itself anymore.
In the longer term, they face a more difficult question.
Because once the patient AI is partnered with Healthdirect controlling intent, triage, safety, governance and routing, and they are spending a lot more time with the patient, how hard will it really be for them to one day build the booking part of the patient journey?
Dr Palit hints at the problem when he says: “If you connect the system properly, the rest follows.”
At this point, while the booking engines would exist still, they would become invisible as far as the patient is concerned.
Potentia won’t be too happy with that assessment.
What all this might mean
The AWS San Diego experiment is not just about the patient journey once they hit a bigger health institution. It’s about controlling and adjusting the journey for system optimisation and patient experience.
In Australia, that journey is moving towards the following layers:
- single front door (patient side AI), hopefully with government, safety, routing and governance inserted (Healthdirect);
- connection, increasingly through clinical workflow networks (referral, advice and guidance); and,
- systems (provider side AI, EMRs, payments, booking, directories).
The future will likely not be defined by any one of these. It might be defined by how they connect however and who controls those connections.
The last word, or the first word of a new world?
If patient-side AI in partnership with something like Healthdirect does become our national front door, and referral networks quietly connect the system underneath, in part to our big institutions using agentic AI to orchestrate the patient journey in and around their shiny giant buildings, then interoperability in Australia may not arrive with the sort of bang you imagine when someone cuts the ribbon on a working national HIE.
Not that a project as risky, expensive and as complicated as a national HIE would ever likely actually go off with a bang. At best the My Health Record lets out a mild crackle and odd pop from time to time.
No, interoperability may just be here one day, built by a few “just doin’ it” type of platforms, institutions and personalities.
All, while some of us are still trying to work out what the ROI on a national HIE might actually be.