

A new report demonstrates that Australia’s fixation with low medicine prices has resulted in the entrenchment of a rigid and controversial pricing tool known as ‘lowest cost comparison’.
A central pillar of Australia’s health technology assessment (HTA) system is comparative evaluation, where a medicine or vaccine is assessed for clinical and economic value against a given comparator.
The current Pharmaceutical Benefits Advisory Committee guidelines state:
“Where there is more than one comparator, the main comparator should be the therapy that prescribers would most replace with the proposed medicine.”
Comparator selection is intended to ensure therapies subsidised under the Pharmaceutical Benefit Scheme deliver additional clinical benefit or cost savings for the healthcare system.
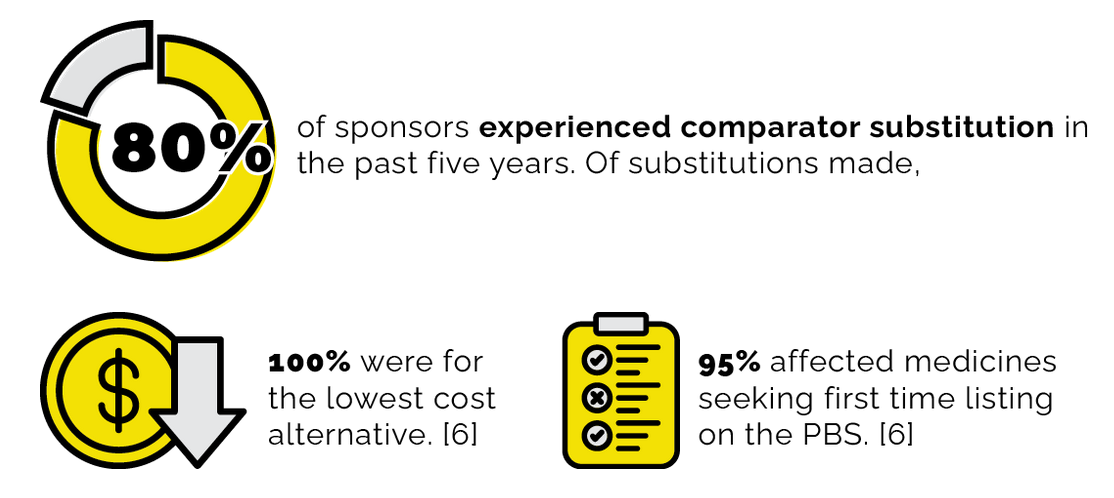
However, over time, comparator selection has increasingly defaulted to the lowest cost comparator (LCC), regardless of alignment with real-world clinical practice.
This trend has resulted in economic assessments anchored to irrelevant therapies, distorting the relationship between the price and value of a medicine.
An economic evaluation in HTA is only valid if it measures the new medicine against what it displaces.
The issue of comparator selection is not new, yet until now, there has been little assessment of its true impact. The cost of comparison: When the benchmark becomes the barrier provides the first independent and comprehensive analysis of this critical issue.
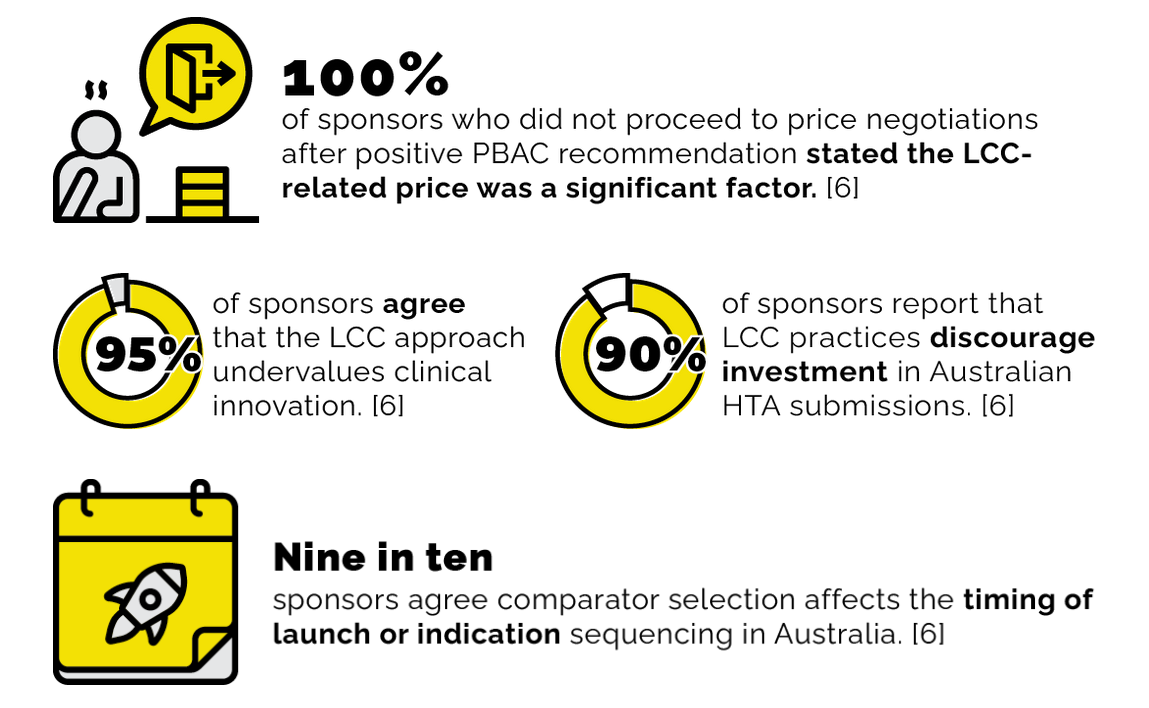
Our analysis finds that LCC has become systemic and now imposes structural barriers to access.
These barriers shape reimbursement outcomes, investment decisions, and Australia’s attractiveness as a launch market for innovation.
These impacts are flowing through to the healthcare system, where clinicians and advocates report patients are experiencing real-world consequences.
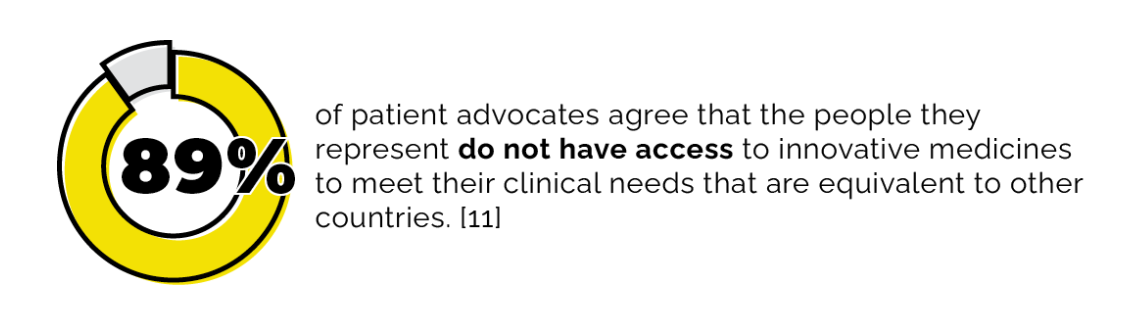
Without access to innovative medicines,
- Australians experience worse physical, psychosocial and financial outcomes,
- Clinical practice is being constrained, and the healthcare system is being put under pressure, and
- Clinical trial activity is at risk, including Australia’s access to emerging innovations.
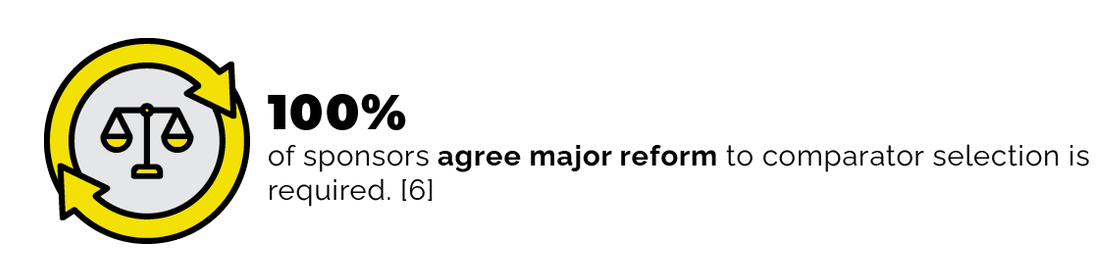
While approaches to fixing comparator selection remain contested, there is strong consensus that reform is necessary, and that the system must move from review to action.
Swift action is now required to secure timely and equitable access to the next generation of medicines.
Evohealth’s phased roadmap proposes eight actions for short-, medium- and long-term reform efforts over the next five years. These reforms are necessary to restore economic and scientific integrity to HTA and re-establish Australia as a credible destination for innovative medicines.
Short term: Contemporise HTA practices in the next 12 months
Medium term: Invest in Australia’s future over the next two years
Long term: Elevate Australia’s global position in the next five years
Renae Beardmore is the managing director of Evohealth.
Deanna Mill, Madeline Wilson, and James Taylor are advisors to Evohealth.
This article was first published by Evohealth. Read the original here.
Also in today’s edition:
- VMOs a $1.3bn black hole, with no value for money found
- Budget preview: what the health sector wants and what it can expect
- NSW Health worker says health system no longer “safe for Jewish people”
- Councils launch wishlist to fix ‘dog’s breakfast’ of rural healthcare
- Existing chronic disease system ‘can’t do it alone’ say $148m grant docs
- If you can’t beat ’em … write the standards
- Beds, mental health and retrievals dominate NT health spend