

Sharing by default comes in on 1 July. Here are the big gaps stopping it from being a brilliant thing, rather than a good start.
I was sitting in a specialist appointment – the kind you wait weeks for and pay a lot to get to – when the data fragmentation problem walked right into the room and sat down next to me.
My respiratory specialist looked at my referral and suggested I get a scan.
I was ready for that. I’d already had one done.
“Where did you get it done?”
And there I was, scrolling through my text messages, trying to find the SMS from the imaging provider telling me my results were ready. I knew it existed. I just couldn’t put my finger on it in the moment, in the chair, slightly flustered, while a very expensive person waited.
Once I found it and said the name, the specialist went straight to that provider’s system and pulled the scan up. It worked. In the moment, it was fantastic.
The UX part of my brain was already twitching.
It only worked because I remembered. Because I could name the provider. Because the imaging provider had cared enough to notify me my results were ready in the first place. Because he happened to have access to that particular system.
I was the search function. I was the interoperability layer.
This is the kind of moment “sharing by default” is meant to fix. From 1 July, the data should be there by default, in one national place. So, I started paying attention to what “by default” actually means, for me and for the people around me.
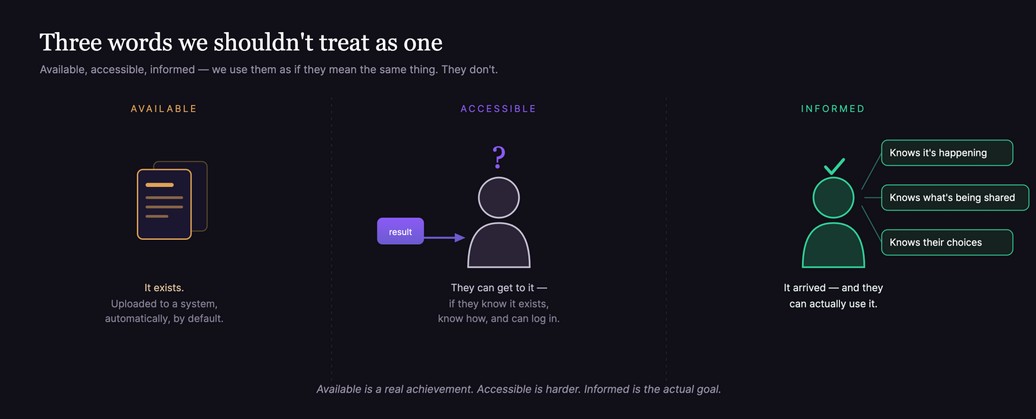
We use three words as if they’re the same thing, and they aren’t:
- Available – the data exists, uploaded somewhere.
- Accessible – the person can actually reach it.
- Informed – the person knows it’s there, understands what it is, and knows the choices they have.
Sharing by default is a huge step on the first. It does much less for the second and third – and those are the ones the patient is left to manage it alone.
Available: what changes on 1 July
From 1 July 2026, the sharing by default reforms mean certain health information will be uploaded to My Health Record automatically – starting with pathology and diagnostic imaging reports.
The Act passed back in February 2025, and this part is enforced: it’s tied to Medicare, so providers can’t treat it as optional.
This is good. I want to say that clearly, because the rest of this article asks questions that matter, and I don’t want them mistaken for cynicism. Moving from a system where uploading was voluntary and patchy to one where it happens by default is real progress.
The fragmentation I described – me as the search function – is part of what this is meant to ease.
It has helped me. I’ve written before about being a patient as much as someone who works in this space – and having my results accessible has changed how I show up to my own care.
I’ve used them to support getting a second opinion. I’ve read through my own results closely enough to catch where a clinician’s judgement was off – because they hadn’t read the report properly.
I’ve prepared proper questions with my doctor ahead of a specialist appointment, instead of walking in cold.
When it works, it’s the difference between being a passenger in your care and being a participant in it. So, none of what follows is me saying this shouldn’t happen. It’s me saying it has to happen well.
And there’s early evidence people are engaging with it.
Australian Digital Health Agency chief digital officer Peter O’Halloran shared at Digital Health Festival, that ahead of the mandate, the number of times “Australians” have viewed this information jumped 112% for pathology and 72% for imaging over the past year.
It’s a big jump. But it counts views. It doesn’t tell you who was viewing – patient or clinician – or whether anyone understood what they saw, or even knew the sharing was happening automatically.
Mr O’Halloran also spoke about the 1800Medicare app – in-app notifications – your phone letting you know when a new report is ready to view. That could close the loop between a result existing and you finding out it exists.
Also in today’s edition:
- Butler arcs up over leadership chances
- Minister ‘confident’ of NDIS reforms despite criticism
- Patients already building their own AI care managers
- Insurers now own 15% of group general practices
- Clinician reticence a bigger AI challenge than consumers
- One in five doctors considering leaving their organisation, Bain report finds
- Surgeons baulk at cannabis driving overhaul
Available isn’t accessible
That works if (1) you know about the 1800Medicare app, (2) connect to your My Health Record in myGov and (3) can get into the app.
Three conditions. All three have to be true. And for a lot of people, not one of them is.
So, I asked around my own family.
My family – I’m from an Asian background – and my partner’s family, who are Australian, have different levels of comfort with technology, different lines of work (aged care to IT). Two have a newborn. Every single one of them has been to a GP, an emergency department, or a hospital. Some have had surgery.
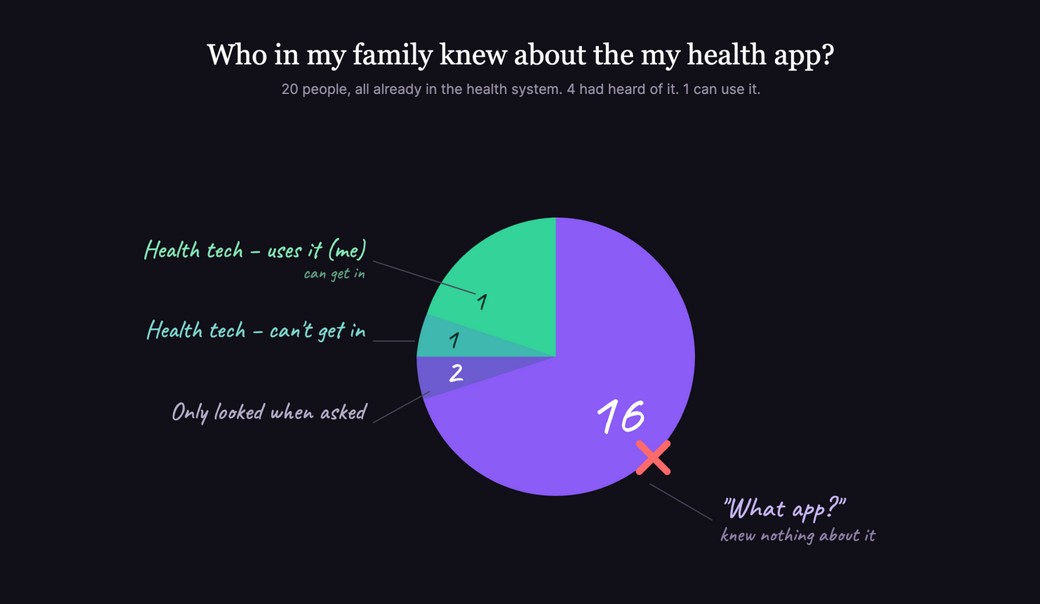
These are not people outside the health system. They are in it. Twenty people. Here’s the breakdown:
Two had looked at the myhealth app when it added eScript functionality – and only because we asked them to, so they could compare it with Scripty (which had done it before the myhealth app did). They don’t actively use it. It doesn’t occur to them to use it.
Two of us work in health tech. One – me – can get in because I’m proactive and actually use it. The other can’t get in at all – a person in health tech.
That’s four out of 20 with any awareness of it.
The other 16? Some version of: “huh – I know Medicare, that’s it. What app?”
Then there’s my mum. She’s the one I actively tried to set up as a carer on my record – someone I want connected to my health information, on purpose. We couldn’t get in. Between us, we couldn’t complete it. And she didn’t really understand what the app was for even once we tried.
Accessible isn’t informed
You can build a system where a patient’s data flows to the right place at the right time – and still have a patient who has no idea it’s happening, what’s being shared, who can see it, or what any of it means.
The infrastructure can be working beautifully while the person at the centre of it is completely in the dark.
We’ve started treating access as the finish line. Results land faster. Reports show up in the app. Views go up. Tick.
But access is the start of the patient’s job, not the end of it. A pathology result you can open the moment it’s ready – before anyone has talked you through it – is more access and potentially more anxiety, if no one’s helping you understand it.
A lot of people don’t know what My Health Record actually is. I can tell you my own family doesn’t. The individual words are fine – “my,” “health,” “record,” sure.
But the concept – that it’s a national system, that their results are being shared into it by default, that there’s a thing they could log into and a choice they could make – that hasn’t landed.
You can’t give informed consent to something you don’t know exists.
I went looking for Australian research on how well consumers actually understand all this. What I found is that most of the awareness research dates back to the old opt-in and opt-out days – years before these reforms.
I couldn’t find current, published work measuring whether Australians understand “sharing by default” specifically: what it shares, what control they keep, what “by default” even means for them.
Think about that.
We’re weeks out from a national change to how everyone’s health information moves, and the numbers being held up are about clicks, not comprehension.
The four gaps I see
1. Sharing by default doesn’t mean looking by default.
Go back to my specialist appointment. The reason the scan moment worked is that I could name the imaging provider, and their system was what told him whether he could access it. So, I asked him directly: would he know to look at My Health Record?
He said no.
The data could be sitting in a national record, uploaded by default – and the specialist told me plainly that My Health Record isn’t where he’d start. The imaging provider’s system is.
The reforms can put a report in a national place.
They can’t, on their own, build the habit of every clinician starting there – the specialist told me as much. And the access log on my own record said the same thing from the other side: when I looked at who’d touched it, it was mostly providers uploading, not clinicians coming in to look.
The system is good at putting data in. Whether anyone pulls it out to use is a different question.
Default sharing is a plumbing change. The habit of looking is a culture change.
They’re not the same project, and the second one is harder. We seem to forget the “change management” part of these health initiatives.
2. The report travels. The images don’t.
Sharing by default covers the written reports from pathology and radiology – not the actual scan images.
The report is often enough, and that’s a great start. But when you’re after a second opinion, the value is often in someone re-examining the images themselves, not inheriting the first read.
So, the patient is often still the one chasing access to the images – or hoping their doctor happens to have access to the imaging provider’s portal, the way my specialist did.
That access isn’t guaranteed; it depends on which provider, which clinic, which arrangement. The fragmentation doesn’t vanish. It moves down a layer.
3. Faster isn’t always better – and that’s OK to say.
Reports are landing in front of patients faster than ever. As it currently stands, most blood and urine pathology and limb X-ray reports are viewable as soon as they’re uploaded; other tests – anatomical pathology and genetic testing, and scans like CT, MRI and ultrasound – sit behind a five-day delay (down from seven).
So, for a lot of results, you can now see them before anyone has talked you through them. That speed solves a real problem – the old days of waiting and wondering. But it creates a new one: a frightened person reading their own result at 9pm, with no one there to make sense of it.
And think about what we’ve been trained to expect.
The current norm is that if something’s wrong, your doctor calls you straight away. It happened with my mum – she had a scan, went and had her lunch, and got a phone call about her results almost immediately. We’ve learned to read “fast contact” as bad news.
Now flip that to a system where the result itself appears straight away. That same trained instinct kicks in – the speed reads as an “uh-oh”, even when there’s nothing wrong at all.
We forget to tell people the most reassuring part: you don’t have to look straight away. It’s okay to wait. It’s okay to leave the result sitting there until your appointment and let your GP walk you through it. Open access should come with that permission attached – not just “here’s your result,” but “here’s your result, there’s no rush, and it’s fine to read this with your doctor instead”.
Giving someone access to their data and giving them the reassurance that they don’t have to face it alone are two different design jobs.
Right now, we’re doing the first and skipping the second.
4. The control you’re promised isn’t always easy to reach.
A lot of the reassurance around all this rests on control: you decide who sees your record, you can see who’s accessed it, you can ask for a report not to be uploaded. Good promises. But look at where they actually live.
You can see who’s accessed your record – but in my experience you can’t check that from the app on your phone. You have to log in to the full record on a desktop browser.
The one feature that lets you hold the system accountable is tucked away from how most people actually use it.
And you can ask for a report not to be uploaded – but you’d have to know to say so before the scan, at the desk, in the moment.
The opt-out appears to be a small “Do not send reports to My Health Record” box on the form, completed by the healthcare professional.
I’ve had a lot of scans and tests – I’m a frequent flyer of these diagnostic and pathology requests – and not once was I asked.
Who tells you that’s a choice? The radiology receptionist? It assumes someone who already knows the system exists, knows their data is about to flow into it by default, and knows they can opt that one report out – possibly for good.
That’s a lot of prior knowledge to expect from a person who just came in for a scan.
Control you don’t know you have, kept somewhere you won’t look, isn’t really control. It’s control on paper.
Related



So what would “informed” actually look like?
The mandate is good. The direction is right.
If we’re going to share by default, I’d like us to inform by default too. That means:
- Telling people, in plain language, that this is happening – including their consent, and their right to say they don’t want something uploaded. Not just relying on healthcare practitioners to have the conversation about My Health Record, privacy and consent – and not leaving it in a portal people struggle to access.
- Measuring understanding and adoption, not just views. A click is not consent, and it certainly isn’t comprehension.
- Giving people permission as well as access – making it clear they can wait and read their results with their doctor rather than alone.
- Better support and implementation – including incentives for software vendors to make it genuinely accessible for consumers to get to this information, not just technically available.
- Co-designing with patients – and not just the ones who show up to consultations or user-testing sessions, but people in community, the ones least likely to be in the room. There’s been co-design with clinicians, specialists and software vendors. The consumer side needs the same depth. The tech matters, sure – but the informed part lives almost entirely in the UX.
- Remembering that the patient is often the only person who’s seen every piece – and building systems that lift that weight off them instead of relying on it.
Connected care isn’t only a data problem. It’s a people-who-are-being-cared-for-problem. And the people at the centre of it deserve to know what’s moving on their behalf.
Available is a real achievement. Accessible is harder. Informed is the actual goal.
We’ve made the data available by default. Now we have to make the person informed by default too.
Mina Giang is co-founder and head of product and experiences at Oexa, a Brisbane-based digital health technology company which created the Scripty app, a consumer-focused, free digital wallet that integrates with the national Active Script List.
This article was first published on Ms Giang’s LinkedIn feed. Read the original article here.